

Most people are familiar with soft contact lenses and glasses, but there is another type of lens that can dramatically improve comfort and vision for people with certain eye conditions. Scleral lenses are larger, rigid gas‑permeable lenses that rest on the white part of your eye (the sclera) rather than directly on the cornea. This design creates a small fluid reservoir over the cornea, which can be therapeutic for a variety of ocular surface problems. In this article we will explain what scleral lenses are, how they work, and who might benefit from them. We will also discuss the advantages and potential drawbacks so you can have an informed conversation with your eye‑care professional.
What Are Scleral Lenses?
A unique design
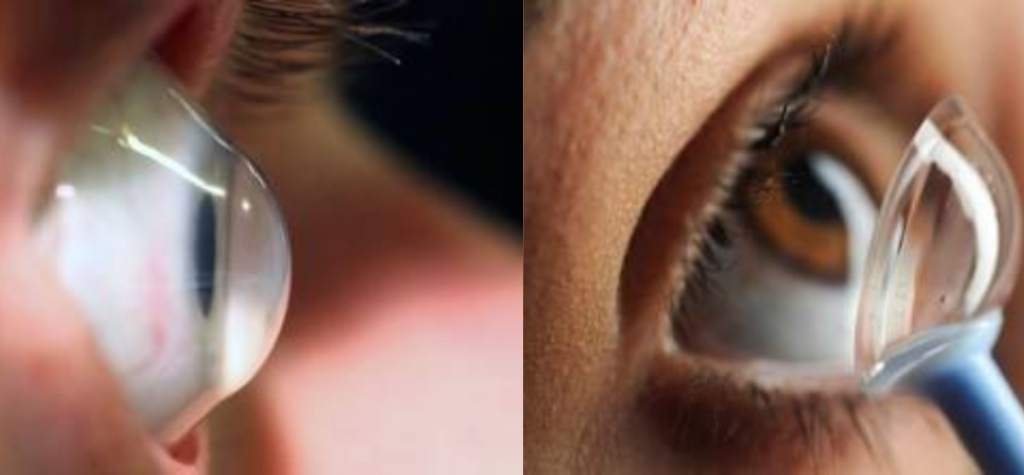
A traditional soft contact lens sits on the clear cornea. Scleral lenses are different. They are rigid gas‑permeable (RGP) lenses measuring 14–24 mm in diameter that vault over the cornea and rest on the sclera. The National Eye Institute (NEI) notes that this design allows a fluid reservoir to form between the lens and the cornea, helping to heal damaged corneas and treat severe dry eye. The American Academy of Ophthalmology (AAO) explains that the success of scleral lenses comes from three features: the precorneal tear reservoir under the lens, protection of the ocular surface, and a smooth refracting surface. Together, these features maintain corneal hydration, promote healing and enhance vision.
Types of scleral lenses
Modern scleral lenses come in several types:
- Full scleral lenses (20–24 mm) – vault over the entire cornea and limbus and rest on the sclera. They provide maximum fluid reservoir and protection.
- Mini‑scleral or semi‑scleral lenses (14–17 mm) – smaller versions that offer the comfort of soft lenses but the optical benefits of rigid lenses.
- Toric and custom designs – spherical, front‑surface toric, back‑surface toric and bi‑toric designs exist to correct astigmatism. Custom CAD‑CAM lenses such as the Boston Scleral Lens Prosthetic Device can include radial channels to facilitate tear exchange.
These variations allow eye‑care professionals to tailor the lens to individual anatomy and visual needs.
How Do Scleral Lenses Work?
The key to the lens design is the fluid reservoir. Because scleral lenses vault the cornea, they create a tiny chamber filled with sterile saline solution. This reservoir keeps the cornea immersed in moisture, shields it from environmental irritants and provides a uniform optical surface. The AAO points out that the reservoir retains tears and protects the cornea from lids and lashes. It also gives the cornea a smooth refracting surface to correct vision.
Rigid materials are used so the lens holds its shape while allowing oxygen to pass through. The Cleveland Clinic notes that scleral lenses are rigid gas‑permeable lenses – often called “hard” lenses – that let oxygen reach the eye. The edges sit under the eyelids, so the lens remains stable and does not move around like smaller contacts.
Benefits of Scleral Lenses

Improved vision and comfort
Scleral lenses correct severe refractive errors that soft lenses cannot. According to the Cleveland Clinic, their greater vision‑correction capabilities and wider coverage help people with high refractive errors obtain clearer, sharper vision. The lenses also resist moving out of position because the edges tuck under the eyelids.
Patients with irregular corneas often experience blurred or distorted vision with regular lenses. The tear reservoir in scleral lenses smooths the corneal surface, providing a stable optical zone and reducing visual aberrations. The systematic review of keratoconus management published in Cureus found that scleral lenses significantly improved best‑corrected visual acuity (BCVA) from a baseline logMAR of 0.50–0.53 to 0.08–0.09 after treatment. The review also reported improved vision‑related quality of life and high patient satisfaction.
Therapeutic reservoir for ocular surface disease
The fluid chamber protects the cornea and promotes healing. The NEI describes how the space between the lens and the cornea can hold fluid to help heal damaged corneas and treat severe dry eye. This continuous moisture is especially helpful for patients with ocular surface disorders such as Stevens–Johnson syndrome, graft‑versus‑host disease or persistent keratitis. The AAO notes that scleral lenses maintain corneal hydration, promote epithelial healing and enhance ocular comfort.
Protecting the eye and delaying surgery
Scleral lenses act as a physical barrier, shielding the cornea from lids, lashes and the external environment. This makes them valuable for patients with recurrent corneal erosions or eyelid disorders. Additionally, the Cleveland Clinic notes that scleral lenses can sometimes help avoid or delay surgeries for conditions like advanced keratoconus.
Stability and comfort in challenging environments
Athletes and people who work in dusty or dry conditions often struggle with soft lenses that dislodge easily or dry out. Because scleral lenses sit under the eyelids and have a sealed fluid reservoir, they remain stable and comfortable. The rigid design provides consistently sharp vision even during rapid eye movements.
Conditions Treated With Scleral Lenses

Corneal ectasia and irregular corneas
One of the primary indications for scleral lenses is corneal ectasia – a group of disorders where the cornea becomes abnormally thin and bulges outward. This includes keratoconus, keratoglobus, pellucid marginal degeneration and post‑LASIK ectasia. The AAO notes that ectatic corneal diseases are among the conditions most successfully managed with scleral lenses. The tear reservoir smooths the irregular cornea, improving vision and comfort.
High refractive errors and astigmatism
People with severe myopia, hyperopia or irregular astigmatism may not achieve adequate vision with glasses or soft lenses. The large diameter of scleral lenses allows them to correct higher refractive errors than standard contacts. The AAO also states that scleral lenses are effective for irregular or high astigmatism.
Ocular surface disease and dry eye
Scleral lenses are often prescribed for ocular surface disorders such as severe dry eye, neurotrophic keratitis, Stevens–Johnson syndrome, ocular cicatricial pemphigoid and graft‑versus‑host disease. The NEI emphasizes that the fluid reservoir helps heal damaged corneas and treat severe dry eye. Patients who experience painful dryness despite maximal medical therapy may find relief with scleral lenses.
Post‑surgical or traumatic corneal irregularities
After corneal transplants or refractive surgery, some patients develop irregular astigmatism or high refractive errors. The AAO lists post‑corneal transplant, pathological myopia, nanophthalmos and post‑trauma corneal irregularities among the conditions treated with scleral lenses. By vaulting over the damaged cornea, the lens can improve vision without further surgical intervention.
Other indications
Scleral lenses are also used for:
- Chemical burns and scarring – they protect healing tissue and improve vision.
- Limbal stem cell deficiency – maintaining moisture aids recovery.
- Medicated ocular therapies – they can hold medicated solutions in the fluid reservoir for extended contact with the cornea.
- Cosmetic or prosthetic purposes – large opaque designs can cover disfigured eyes.
Potential Drawbacks and Risks
While scleral lenses offer many benefits, they are not without downsides.
Cost and fitting time
Fitting scleral lenses requires specialized equipment and expertise. The manufacturing and fitting process often involves several visits to adjust the lens design. The Cleveland Clinic notes that most people go through two or three attempts to get the right fit. Custom lenses are more expensive than standard contacts, and costs can be higher if insurance does not cover them.
Learning curve and handling issues
Scleral lenses are larger than regular contacts, so learning to insert and remove them takes practice. The Cleveland Clinic explains that people may need to start with short wear times and gradually increase them. The systematic review on keratoconus reported that handling issues were one of the most common complications, occurring in 10–63 percent of patients. Fogging is another issue; about 58 percent of patients in the review experienced lens fogging.
Maintenance and risk of infection
Because particles can accumulate in the fluid reservoir, most wearers need to remove and clean the lens at least once during the day. Proper hygiene is vital. The Cleveland Clinic emphasizes that wearers should never use tap water or saliva to clean the lenses. Failure to follow cleaning instructions can lead to infections or corneal damage.
Contraindications
Scleral lenses are not appropriate for everyone. The AAO warns that corneal edema and compromised endothelial function are contraindications because scleral lenses can worsen swelling. Severe ocular allergies or inflammation may also prevent successful lens wear. Always consult an eye‑care professional to determine if scleral lenses are suitable for you.
Who Needs Scleral Lenses?
Scleral lenses are prescribed for a variety of conditions, but they are not a cure‑all. If you fall into one of the following categories, talk to your eye doctor about whether you might benefit from scleral lenses:
- People with keratoconus or other corneal ectasias – to achieve clear vision and postpone or avoid corneal transplants.
- Individuals with severe dry eye or ocular surface disease – to maintain constant moisture and promote healing.
- Patients with irregular astigmatism or high refractive errors – when glasses and soft lenses cannot provide adequate vision.
- Post‑surgical or trauma patients – to correct irregularity after corneal transplant, LASIK, injury or chemical burns.
- Athletes and active individuals – who need stable, clear vision and protection in challenging environments.
- Wearers with poor tolerance to soft or hybrid lenses – who experience discomfort or lens displacement.
Always have a thorough evaluation with an optometrist or ophthalmologist experienced in scleral lens fitting. They will assess corneal health, tear film, and eyelid function, and may use diagnostic tools such as optical coherence tomography to ensure an optimal fit.
The Fitting Process

Consultation and measurements
Your eye‑care provider will examine your eyes and discuss your visual needs. They may use corneal topography or tomography to map the shape of your cornea and sclera. Based on these measurements, a trial lens is selected, and the fit is assessed under a slit‑lamp microscope. Adequate clearance over the cornea and limbus without excessive bubbles or compression is important.
Custom fabrication
Most scleral lenses are custom‑made. Computer‑aided design (CAD) and lathing technology allow precise tailoring of the lens shape, size and curvature. This ensures even pressure distribution and minimal movement. Your practitioner may order one or more lenses before achieving the best fit.
Training and follow‑up
You will learn how to insert and remove the lens using a “tripod” technique and how to fill it with non‑preserved saline. The Cleveland Clinic suggests overfilling the lens with saline to avoid trapping air bubbles. Regular follow‑up visits are essential to monitor corneal health and address any issues. Many patients adjust to the lenses within a few weeks, but some may need longer to reach full‑day wear.
Care and Maintenance Tips
To maximize safety and comfort:
- Use appropriate solutions. Clean the lenses with recommended RGP cleaning solution, rinse with sterile saline and disinfect according to your doctor’s instructions. Avoid tap water, saliva or homemade saline.
- Handle lenses with clean hands. Always wash and dry hands before touching the lenses.
- Replace lenses periodically. Scleral lenses usually last one to two years. Replace them sooner if they become damaged.
- Watch for discomfort. If you experience persistent pain, redness or decreased vision, remove the lens and contact your eye‑care provider.
- Take breaks. Remove the lens during the day if fogging occurs, clean it and reapply with fresh saline.
Comparing Scleral Lenses With Other Contact Lenses
Soft contact lenses
Soft lenses are comfortable and easy to use but may dry out quickly and cannot correct severe refractive errors. They rest on the cornea and move with each blink. Scleral lenses, being rigid, provide sharper optics and remain stable. The trade‑off is the learning curve and higher cost.
Hybrid lenses
Hybrid lenses have a rigid center and soft skirt. They combine the optical quality of RGP lenses with the comfort of soft lenses and work well for mild irregular corneas. However, they may still move or dry out more than scleral lenses and cannot provide the same level of moisture reservoir.
Ortho‑K lenses
Orthokeratology lenses are worn overnight to reshape the cornea temporarily. They are primarily used to slow myopia progression or provide daytime vision without correction. They do not offer the therapeutic benefits of scleral lenses and are unsuitable for treating ocular surface disease.
Prosthetic/cosmetic lenses
Decorative lenses change the appearance of the eye and sometimes correct vision. They do not have therapeutic reservoirs and should always be prescribed to avoid complications.
Conclusion and Takeaway
Scleral lenses are an innovative solution for people with challenging vision and ocular surface problems. By vaulting over the cornea and holding a reservoir of saline, these large rigid lenses can provide clear, stable vision and relief from severe dry eye and other conditions. They are particularly useful for patients with corneal ectasias, high refractive errors, or ocular surface diseases. However, they require specialized fitting, diligent care and a learning curve. Work closely with an eye‑care professional to determine if scleral lenses are right for you. With the proper fit and maintenance, scleral lenses can transform your visual comfort and quality of life.
{kind=link}