

A New Horizon for Vision Restoration
Imagine being told you will never read your favorite book again. For millions of people worldwide living with advanced age‑related macular degeneration (AMD) or inherited conditions such as retinitis pigmentosa, profound vision loss has been a life‑altering reality. For decades, researchers have dreamed of creating a bionic eye that could restore sight by replacing damaged photoreceptors with electronic implants. Early devices offered only light perception and crude patterns, but a new generation of retinal implants is changing that narrative. In late 2025 a tiny wireless chip called PRIMA helped dozens of people with geographic atrophy (a severe form of AMD) regain the ability to read books and navigate subway signs. This article explores how bionic eyes work, chronicles the evolution of vision prostheses, examines the recent upgrades making headlines, and looks ahead at what the future may hold.
What Is a Bionic Eye?

A bionic eye is not a glass prosthesis that simply sits in the orbit; it is a sophisticated electronic system designed to restore partial vision by stimulating the visual pathway. Unlike eyeglasses or contact lenses that correct refractive errors, bionic eyes bypass damaged photoreceptors and send signals directly to surviving retinal neurons, the optic nerve or even the visual cortex. The latest review of the field notes that the primary approaches include retinal implants, optic nerve stimulation and cortical visual prostheses. Retinal implants have shown the most clinical progress, with devices such as Argus II and Alpha AMS demonstrating that people with severe retinitis pigmentosa can perceive light, detect motion and recognize large objects. However, early devices offered low resolution and narrow fields of view; ongoing research aims to increase electrode density, improve biocompatibility and integrate artificial intelligence to process images more like the natural eye.
How a Bionic Eye Works
Most bionic eye systems share a three‑part architecture:
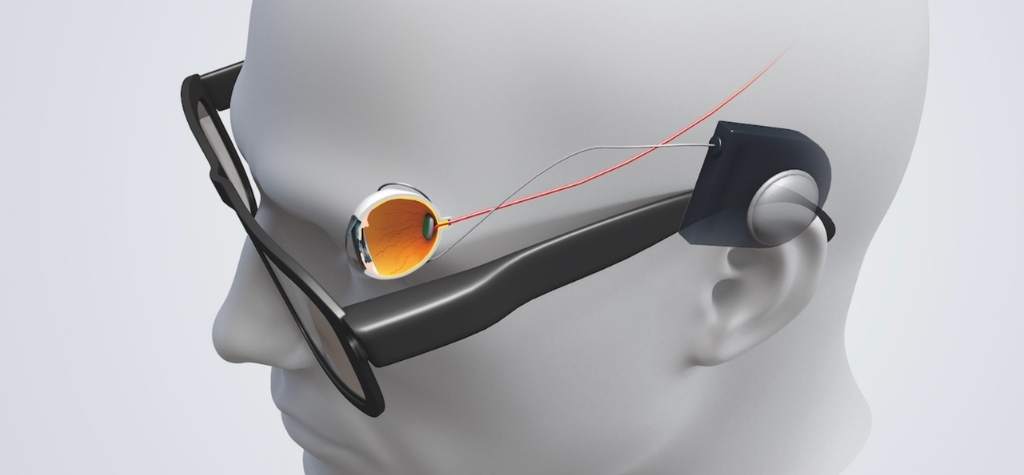
- External vision capture: A miniature video camera mounted on glasses captures the world in real time. The Argus II system, for example, uses a small camera and transmitter mounted on a pair of sunglasses.
- Image processing: A belt‑mounted or pocket‑sized processing unit converts these images into digital signals and often enhances contrast, brightness or zoom. In the PRIMA system, the glasses project infrared patterns onto a tiny chip implanted under the retina.
- Neural stimulation: The implant converts the incoming signals into electrical pulses that stimulate surviving retinal cells or cortical neurons. The user perceives these pulses as patterns of light (phosphenes) that, with training, can convey shapes, letters and orientation cues.
Different implants target different parts of the visual pathway:
- Epiretinal devices, like Argus II, sit on the retinal surface and stimulate ganglion cells via a 60‑electrode array.
- Subretinal implants, such as Alpha AMS and PRIMA, replace degenerated photoreceptors by stimulating bipolar cells from within the retina. PRIMA uses photovoltaic pixels that require only light energy to function.
- Suprachoroidal implants are positioned between the retina and the sclera. The second‑generation Australian bionic eye uses a 44‑electrode array surgically implanted behind the eye and is coupled to a camera on glasses.
- Cortical implants bypass the eye entirely by placing electrodes directly on the visual cortex. Devices like Orion deliver patterns of light via electrodes implanted in the brain and can help people with no eyes or severely damaged optic nerves.
The Evolution of Bionic Eye Technology
Argus II: The First FDA‑Approved Retinal Prosthesis
The bionic eye story began in the early 2000s with Second Sight Medical Products and its Argus epiretinal prosthesis. Argus I allowed patients to perceive light; Argus II followed with 60 electrodes that could create simple patterns of light. In February 2013, the U.S. Food and Drug Administration (FDA) approved Argus II as the first implanted device to treat adults with advanced retinitis pigmentosa. The system comprises a video camera and transmitter on glasses, a video processing unit, and an implanted array on the retina. Patients using Argus II report being able to distinguish light from dark, identify doorways, sort laundry and detect large objects. However, the low electrode count means vision remains coarse, and the manufacturing company discontinued the device in 2019.
Alpha IMS and Alpha AMS: High‑Density Subretinal Chips
German firm Retina Implant AG pioneered the Alpha series of subretinal implants. Alpha IMS, tested in the early 2010s, required an external power supply. Its successor Alpha AMS incorporated a wireless microphotodiode array (MPDA) with ~1,600 electrodes to stimulate bipolar cells, eliminating the need for a bulky external power cable. Clinical trials showed that Alpha AMS could enable users to detect light, recognize shapes and read large letters, although electrode corrosion and immune reactions posed challenges. Regulatory approvals were obtained in Europe, but the company dissolved in 2019, leaving the technology in the hands of academic partners.
The Australian Suprachoroidal Prosthesis: 44 Electrodes and Improved Navigation
Researchers from the Bionics Institute, Centre for Eye Research Australia (CERA) and the University of Melbourne developed a suprachoroidal retinal prosthesis. The device’s 44‑electrode array is implanted behind the retina and receives signals from a camera on glasses, delivering electrical pulses to stimulate retinal cells. In a clinical trial that implanted four people with retinitis pigmentosa in 2018, the device remained stable and durable for more than 2.7 years, with 97 % of electrodes still functioning. Patients reported improved navigation, the ability to locate doorways and objects on tabletops, and greater confidence in moving through new environments. Researchers aim to develop a third‑generation device with more electrodes and refined vision processing.
Cortical Implants: When the Eye Is No Longer Viable
For people whose eyes or optic nerves are too damaged for retinal implants, cortical prostheses offer hope. The Orion Visual Cortical Prosthesis System, developed by Cortigent (formerly Second Sight), uses a camera and processor similar to Argus II but sends the signals wirelessly to a 60‑electrode array implanted on the visual cortex. In a U.S. early feasibility study that began in 2017, six profoundly blind participants underwent implantation. Five years later, the three participants still using the system have reported no device malfunctions and continue to use the device at home and in their communities. Efficacy evaluations showed participants performed better at localizing light and identifying motion with the system turned on versus off. A functional low‑vision assessment indicated improved real‑world tasks such as navigating a sidewalk and sorting laundry. Cortigent plans to begin pivotal clinical trials in the coming years.
Other brain‑computer interface companies are also exploring visual cortical implants. Neuralink’s experimental Blindsight system uses 36 flexible threads sewn into the visual cortex; a camera sends images to a smartphone, which converts them into signals delivered to the brain. As of mid‑2026, human trials are anticipated, though independent researchers caution that the high electrode count may not translate to high‑quality vision. Another project, the Intracortical Visual Prosthesis (ICVP), uses a 400‑electrode implant and has helped a person with retinal damage navigate and perform basic tasks two years after implantation.
Spotlight on PRIMA: A Photovoltaic Leap Forward
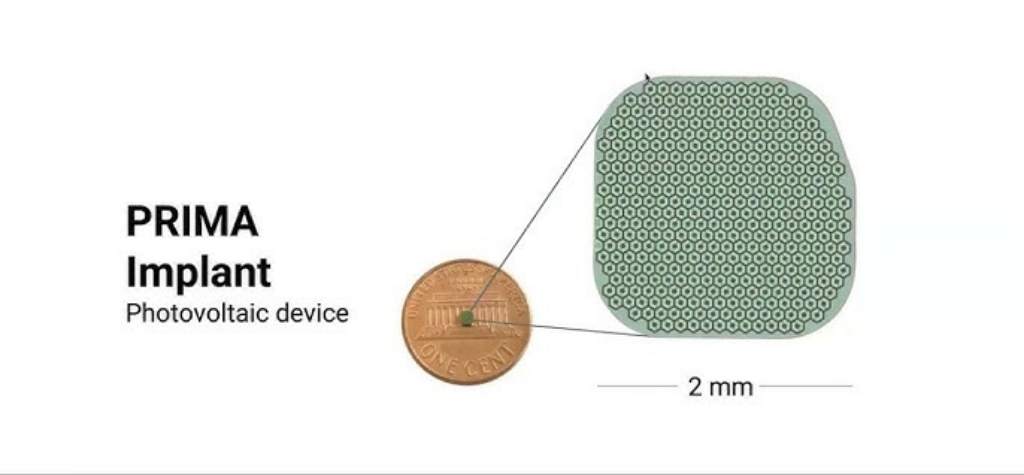
The bionic eye making headlines in late 2025 is PRIMA, a photovoltaic subretinal prosthesis developed by Science Corporation and researchers at Stanford University. PRIMA builds on the lessons of Alpha AMS but adopts a wireless, light‑powered design. Each implant is a thin 2 × 2 millimetre silicon chip only 30 micrometres thick that contains 378 photovoltaic pixels. These tiny pixels convert near‑infrared light projected from special glasses into electric pulses that stimulate bipolar cells in the degenerated retina. Because the implant is photovoltaic, no external power cable is needed, and the chip can be implanted under the retina through a minimally invasive surgery.
How PRIMA Works
- An integrated camera mounted on the glasses captures visual scenes and projects them as near‑infrared patterns onto the implanted chip.
- Each pixel acts like a tiny solar cell, generating a current that stimulates the surrounding retinal neurons.
- The chip’s design allows patients to combine their natural peripheral vision with the prosthetic central vision, improving orientation and navigation.
According to Daniel Palanker, one of the device’s inventors, previous prosthetic devices only allowed users to detect light; PRIMA is the first to provide form vision. Palanker imagined the concept two decades ago, noting that the eye’s transparency could be exploited to deliver information via light. Today, that idea is helping patients read again.
Clinical Trial Results: Reading Again
The pivotal PRIMAvera study enrolled 38 participants aged over 60 with advanced geographic atrophy due to dry AMD. The trial was conducted across 17 centers in Europe and evaluated safety and efficacy at 6‑ and 12‑month intervals. Key findings include:
- Improved visual acuity: At 12 months, 81 % of participants (26 of 32 who reached this point) achieved a visual acuity improvement of at least 10 letters (logMAR 0.2) compared with baseline. The improvement was highly significant (p < 0.001). Peripheral natural vision did not decline.
- Meaningful reading: In Stanford Medicine’s summary of the trial, 27 of 32 participants regained the ability to read one year after implantation. Some participants could read with acuity equivalent to 20/42 thanks to digital enhancements such as zoom and contrast adjustments.
- Average gain: On average, participants improved by five lines on a standard eye chart; one person improved by 12 lines. Participants reported using the device for daily tasks such as reading books, food labels and subway signs.
- Safety profile: During the PRIMAvera study, 26 serious adverse events occurred in 19 participants, mainly within the first two months; 95 % resolved within two months. Common issues included ocular hypertension, peripheral retinal tears and subretinal hemorrhage. No participants lost peripheral vision.
The PRIMA system allows users to adjust contrast and magnification on their glasses and can deliver up to 12× zoom. Early adopters report that tasks like reading food labels and navigating subway systems have become possible again.
Why PRIMA Represents an Upgrade
PRIMA’s performance highlights several advantages over previous bionic eyes:
- Wireless power and high pixel count: The photovoltaic design eliminates cables and external power sources. Its 378 pixels are still fewer than the human eye’s millions of photoreceptors but far more than the 60‑electrode Argus II, allowing for more detailed vision.
- Integration of natural vision: Patients retain peripheral vision because the near‑infrared projection does not stimulate intact photoreceptors; prosthetic and natural inputs merge seamlessly.
- Digital enhancements: The ability to adjust contrast and zoom gives users better control and may compensate for low pixel counts.
- Modular upgrade path: Because the implant operates wirelessly, it can potentially be replaced with future chips that have smaller pixels and higher resolution. Researchers are already developing a next‑generation chip with 20 micron pixels and 10,000 pixels per chip, which could deliver 20/80 vision and approach 20/20 with digital zoom.
Other Vision Restoration Technologies in Development

Brain–Computer Interfaces and Blindsight
The BrightFocus Foundation notes that in addition to retinal implants, developers are testing brain implants that bypass the eye entirely. Neuralink’s Blindsight uses 36 flexible threads containing roughly 3,000 electrodes to deliver visual signals directly to the visual cortex. A camera on glasses sends images to a smartphone, which converts them into signals transmitted wirelessly to the brain. Early testing on animals has shown some success, and human trials are planned for 2026. Other research groups have implanted a 400‑electrode intracortical visual prosthesis that has helped a person who lost vision due to retinal detachment perform everyday tasks two years after surgery.
Suprachoroidal Prostheses and New Electrode Arrays
The second‑generation suprachoroidal prosthesis from Bionic Vision Technologies uses a 44‑electrode array and has shown functional vision improvements and long‑term stability. Participants could locate doorways, avoid obstacles and find items on table‑tops, gaining confidence to explore new environments. The team plans to increase electrode count and refine vision processing for the generation 3 device.
Artificial Retina with Nanowire Arrays
BrightFocus reports that scientists have developed artificial eyes using nanowire arrays. These nanowires are tens of thousands of times thinner than a human hair and can be packed more densely than natural photoreceptor cells. Although the 2020 Nature paper demonstrating this technology represented a breakthrough, researchers cautioned that connecting these artificial retinas to the optic nerve or visual cortex remains a major challenge.
Retinal Implants Market and Discontinued Devices
While early devices like Argus II proved the concept, commercial adoption has been limited due to high cost and technical challenges. Argus II was discontinued, and the Alpha AMS program was paused when Retina Implant AG dissolved in 2019. The latest review emphasises that high costs, regulatory hurdles and long‑term implant stability remain significant barriers to widespread adoption. Nevertheless, the field is progressing quickly thanks to interdisciplinary collaborations and advances in materials science, wireless power, and artificial intelligence.
Living with a Bionic Eye: Patient Experiences
Regaining Reading and Independence
For many participants in the PRIMA trial, the biggest joy has been reading again. After training, 27 of 32 participants regained the ability to read letters on an eye chart. Some achieved acuity close to 20/42 with digital enhancements. Participants have reported reading books, food labels and subway signs with the device. Because the glasses allow them to adjust contrast and magnification, users can tune the image to suit their needs, similar to adjusting font size on an e‑reader.
Navigating the World with Suprachoroidal Implants
Participants in the Australian suprachoroidal trial reported improved orientation and mobility. They could locate doorways, avoid obstacles and find objects such as items on a table. They also reported greater confidence exploring new environments and reduced need for assistance when travelling to local shops. Such improvements supplement the use of canes or guide dogs rather than replace them. In addition, the implants remained stable, with 97 % of electrodes functioning after 2.7 years, suggesting good long‑term reliability.
Daily Life with Argus II and Orion
Patients who received Argus II described being able to detect doorways, windows, curbs and large objects. Some reported sorting laundry by color or recognizing stove burners, tasks that require awareness of shapes and contrasts. Because the field of view is limited to the implant area, users still rely on mobility aids for safety. In the Orion feasibility study, participants were observed at home performing daily activities like navigating sidewalks and sorting laundry. All reported positive real‑world benefits when the system was on compared with off. Importantly, the device did not malfunction over five years and serious adverse events were rare.
Training and Adaptation
Using a bionic eye is not as simple as flipping a switch. Patients undergo extensive training to interpret the dots of light that make up their prosthetic vision. For PRIMA, participants began using the glasses four to five weeks after surgery and trained for months to reach top performance. This is comparable to the time required for cochlear implant recipients to learn how to interpret electronic sounds. Patients also need regular adjustments of software and hardware, and they often work with low‑vision rehabilitation specialists to integrate the prosthetic input with remaining natural vision.
Challenges and Ethical Considerations

Technical and Biological Hurdles
Even with recent advances, bionic eyes face significant challenges. Early devices suffer from low resolution; Argus II’s 60 electrodes produce coarse images, while PRIMA’s 378 pixels still fall short of natural vision’s million‑pixel resolution. Long‑term biocompatibility and electrode stability remain concerns; subretinal devices like Alpha AMS can experience electrode corrosion or immune responses. For cortical implants, surgical risks include infection, inflammation and potential cognitive side effects. Moreover, all implants require invasive surgery, which may not be feasible for frail patients.
Cost and Accessibility
Most bionic eyes cost tens or hundreds of thousands of dollars and are approved only for small patient populations. Argus II was approved under a humanitarian device exemption for fewer than 10,000 patients in the United States. Insurance coverage is limited, and maintenance costs (e.g., upgrades, repairs, training) can be high. The PRIMA system is currently under review for CE mark approval in Europe and has not yet received U.S. approval. Wide availability will depend on successful pivotal trials and regulatory approvals in different regions.
Patient Expectations and Informed Consent
Clinicians emphasize the need to manage expectations. Bionic eyes do not restore natural vision; they provide a crude, low‑resolution representation of the world that requires practice to interpret. Patients must understand that surgery carries risks, that training is lengthy and that the device may not work for everyone. There is also an ethical responsibility to ensure that early adopters are supported if companies fail or devices become obsolete — a reality underscored by the discontinuation of Argus II.
Equity and Global Impact
Visual impairment disproportionately affects people in low‑ and middle‑income countries, where access to health care and advanced technology is limited. While bionic eyes offer hope, the technology must be developed with equitable access in mind. Additionally, prevention and treatment of conditions like AMD, retinitis pigmentosa, diabetic retinopathy and glaucoma remain critical. Bionic eyes should not divert attention from proven public health interventions but rather complement them.
The Road Ahead: From Pixels to Perception
The future of bionic eye technology is filled with promise. Researchers are working to:
- Increase pixel density and resolution. PRIMA’s next‑generation chip will have 10,000 pixels, potentially improving acuity to 20/80 or better. Other groups are experimenting with nanowire arrays that could surpass natural photoreceptor density.
- Improve materials and biocompatibility. Advances in electrode materials may reduce immune reactions and extend implant life.
- Incorporate artificial intelligence and machine vision. AI algorithms could optimize image processing, enhance contrast and identify important objects in real time. Neural networks may learn to predict the user’s intentions or highlight hazards.
- Develop hybrid approaches. Combining bionic implants with gene therapy, optogenetics or stem‑cell therapy may allow some patients to regain natural photoreceptors while using electronics for additional vision.
- Expand cortical prostheses. Projects like Orion, Blindsight and ICVP aim to help people with optic nerve damage or no remaining eyes. Brain‑computer interfaces could one day provide direct visual input to the brain, although safety and ethical considerations must be addressed.
- Enhance rehabilitation and user experience. Future devices may integrate augmented reality overlays, voice commands and haptic feedback to make prosthetic vision more intuitive and immersive.
As these innovations advance, collaboration among engineers, ophthalmologists, neuroscientists and ethicists will be essential. Ensuring that patients have access to training and follow‑up care, and that devices remain upgradable and supported, will help avoid the pitfalls seen with earlier devices.
Conclusion: A Glimpse of Light
The idea of a bionic eye has transitioned from science fiction to clinical reality. Early devices like Argus II proved that electronic implants could restore basic light perception, but limitations in resolution and reliability curtailed adoption. Subretinal and suprachoroidal implants increased electrode counts and improved safety, enabling users to recognize shapes and navigate. Cortical implants opened the door for people with severely damaged eyes. Now, with the PRIMA upgrade, dozens of people with advanced AMD can read again, regaining independence and quality of life.
Bionic eyes are still in their infancy. The journey from 60 electrodes to thousands of pixels mirrors the evolution of cochlear implants and suggests that visual prostheses will continue to improve. Still, these devices are not a cure for blindness; they offer partial vision and require significant training. Ethical considerations around cost, accessibility and long‑term support remain paramount. As we stand at the dawn of an era where blind people are seeing again, continued research, collaboration and compassion will determine how widely and equitably this technology transforms lives.
{kind=link}