

Why care about diabetic retinopathy?
Millions of people across the world live with diabetes. This chronic condition doesn’t just affect blood sugar; it can also damage the tiny blood vessels that feed the light‑sensing tissue at the back of your eye. That damage is called diabetic retinopathy, and it’s one of the leading causes of preventable blindness in adults. By understanding how diabetic retinopathy develops, who is at risk and how it is treated, you can take steps to protect your vision.
Stat alert: Health authorities estimate that more than half of all people with diabetes will develop some degree of diabetic retinopathy during their lifetimenei.nih.gov. In 2020, about 103 million people worldwide were living with the condition, and projections suggest that number could jump to 160 million by 2045.
In this long‑form guide we’ll break down everything you need to know about diabetic retinopathy. You’ll learn what it is, how it affects the eye, who is at risk, warning signs to watch for, diagnostic tools, current treatments and what you can do today to lower your risk. Short paragraphs, clear language and handy lists make it easy to follow along, even if you’ve never studied eye health before.
Understanding diabetic retinopathy
What is diabetic retinopathy?
Diabetic retinopathy is a complication of diabetes that damages the retina—the thin layer of light‑sensitive tissue at the back of your eye. High blood sugar levels over time cause changes in the small blood vessels in the retina. These vessels may weaken, leak or become blocked. In later stages new abnormal vessels grow (a process called neovascularization). These fragile vessels break and bleed easily, leading to scar tissue and possible retinal detachment. Without treatment, the damage can lead to vision loss or blindness.
The U.S. National Eye Institute (NEI) explains that high blood sugar can cause tiny retinal blood vessels to swell, leak or close off. To compensate, the eye sometimes grows new vessels that are abnormal and leak even more. This combination of vessel damage, leakage and growth is the hallmark of diabetic retinopathy.
How diabetes damages the retina
Inside your eye, the retina turns light into electrical signals that travel along the optic nerve to your brain. Those signals allow you to see. For the retina to work properly, it needs a constant supply of oxygen and nutrients delivered by a network of microscopic blood vessels. Chronically high glucose injures this delicate network in several ways:
- Glucose converted to toxic compounds: Long‑term high sugar triggers alternative metabolic pathways (the polyol pathway) and forms harmful advanced glycation end products (AGEs). These chemicals stiffen vessel walls and slow blood flow.
- Inflammation and oxidative stress: Hyperglycemia prompts inflammation and oxidative stress, which further weakens blood vessels and encourages abnormal vessel growth.
- Protein kinase C (PKC) activation: Elevated glucose activates PKC, causing vessels to leak and causing the retina to become swollen and thickened.
Over time, these factors lead to ischemia (lack of oxygen) in parts of the retina. The body responds by releasing growth factors that promote new vessel growth (neovascularization). Unfortunately these new vessels are fragile, bleed easily and can pull on the retina, sometimes leading to retinal detachment.
Who is at risk for diabetic retinopathy?
Everyone with diabetes—type 1, type 2 or gestational—can develop diabetic retinopathy. According to the NEI, the risk rises the longer you’ve had diabetes; more than half of people with diabetes will develop some level of retinopathy. Certain factors increase the odds or speed up progression:
- Duration of diabetes: The longer you live with diabetes, the higher the risk. People who have had diabetes for 20 years or more have a much greater chance of developing retinopathy.
- High blood sugar levels: Poorly controlled blood glucose damages the retina. Keeping blood sugar near your target range is one of the most effective ways to reduce risk.
- High blood pressure and high cholesterol: Hypertension and elevated lipid levels strain blood vessels and accelerate damage.
- Kidney disease: Diabetic nephropathy often goes hand in hand with retinopathy. A weakened kidney suggests other vascular complications.
- Pregnancy: Women who already have diabetes or who develop gestational diabetes during pregnancy are at higher risk. The hormonal changes of pregnancy can worsen retinopathy; pregnant women with diabetes should have a comprehensive eye exam early in pregnancy.
- Puberty and adolescence: Rapid hormonal changes during puberty may increase risk.
- Obesity and lack of exercise: Being overweight, physically inactive or having metabolic syndrome raises the risk of diabetes and its complications.
Other emerging risk factors include chronic inflammation, low vitamin D levels, oxidative stress and genetic predispositions. While you can’t control your genes, you can manage modifiable risks such as blood pressure and cholesterol.
Global prevalence
A systematic review on diabetic retinopathy concluded that about 93 million people worldwide have diabetic retinopathy, and nearly 25–30 % of those develop diabetic macular edema (DME). In the United States, projections predict 16 million people could have diabetic retinopathy by 2050, with 3.4 million experiencing vision‑threatening complications. Those numbers highlight why early diagnosis and treatment are critical.
The stages of diabetic retinopathy

Diabetic retinopathy develops slowly. Eye doctors classify it into two broad stages—non‑proliferative diabetic retinopathy (NPDR) and proliferative diabetic retinopathy (PDR)—with several sub‑stages in between.
Non‑proliferative diabetic retinopathy (NPDR)
NPDR is the early stage. Blood vessels in the retina become weak and leak small amounts of blood or fluid. The leakage forms tiny, round outpouchings called microaneurysms. NPDR is divided into three severity levels:
- Mild NPDR: Only a few microaneurysms or small leaks. There may be cotton wool spots (areas of nerve fiber damage) or hard exudates (yellowish lipid deposits) in the retina.
- Moderate NPDR: More retinal blood vessels become blocked or leaky. You might see dot or blot hemorrhages, venous beading or intraretinal microvascular abnormalities.
- Severe NPDR: Many blood vessels are blocked, depriving large sections of the retina of oxygen. This stage is a warning sign that proliferative retinopathy may develop soon.
Diabetic macular edema (DME), a swelling in the central retina (macula), can occur at any stage of NPDR. DME develops when leaking fluid collects in the macula, causing central vision to blur. Cleveland Clinic notes that DME can be center‑involved (affecting the center of the macula) or non‑center‑involved. Center‑involved DME is a leading cause of vision loss in diabetic retinopathy.
Proliferative diabetic retinopathy (PDR)
PDR is an advanced, sight‑threatening stage. When the retina becomes severely deprived of oxygen, it releases signals that trigger abnormal new vessel growth. These new vessels grow on the surface of the retina and into the vitreous gel. Because they are fragile and abnormal, they may break and bleed. Scar tissue can form and pull on the retina, leading to tractional retinal detachment. The American Academy of Ophthalmology (AAO) stresses that these complications can cause severe vision loss or blindness.
PDR can be described as early PDR (some new vessels but no high‑risk characteristics) or high‑risk PDR (new vessels accompanied by vitreous hemorrhage or near the optic nerve head). High‑risk PDR requires urgent treatment to prevent permanent vision loss.
Symptoms – what to watch for
One of the dangers of diabetic retinopathy is that it often develops without noticeable symptoms in the early stages. By the time you notice changes in your vision, retinopathy may already be advanced. Common symptoms include:
- Blurry or distorted vision.
- Floaters—dark spots or strings that drift across your vision.
- Vision that changes from blurry to clear and back again.
- Dark or empty spots in your field of view.
- Difficulty seeing at night.
- Colors appearing faded or washed out.
- Sudden loss of vision or persistent blank areas.
The AAO warns that floaters, fluctuating vision and poor night vision can signal diabetic retinopathy aao.org. Because early stages may be symptom‑free, regular eye exams are essential for anyone with diabetes.
Diagnosis – how doctors detect diabetic retinopathy

Dilated eye exam
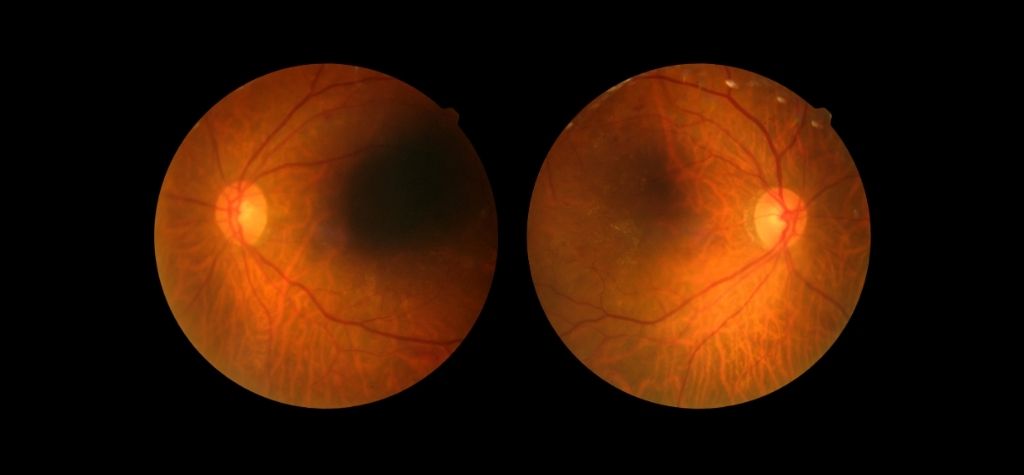
The simplest and most important diagnostic tool is a comprehensive dilated eye exam. An ophthalmologist or optometrist dilates (widens) your pupils using special eye drops. This allows them to see the retina more clearly and look for signs of retinopathy such as microaneurysms, hemorrhages and new vessel growth. The Cleveland Clinic notes that early changes—including cotton wool spots and retinal hemorrhages—are visible during a dilated exam.
Imaging tests
If your doctor spots signs of diabetic retinopathy or needs to monitor progression, they may order imaging tests:
- Optical coherence tomography (OCT): This non‑invasive scan uses light waves to create high‑resolution cross‑sectional images of the retina. OCT can detect macular edema (swelling) and measure its thickness. The AAO lists OCT as a key tool for evaluating DME.
- Fundus photography: A special camera takes detailed photographs of the retina to document changes over time.
- Fluorescein angiography: A dye is injected into a vein in your arm. As the dye flows through the eye, a camera captures images. This helps doctors see leaking or blocked blood vessels and new vessel growth.
Tele‑ophthalmology and artificial intelligence
Advances in technology are improving access to screening. Tele‑ophthalmology uses digital retinal photos taken in primary care clinics or pharmacies. These images are sent to an ophthalmologist or optometrist for review. A systematic review found that tele‑screening programs have increased access to eye care for people in rural or underserved areas. Remote screening is particularly valuable because fewer than half of people with diabetes receive regular eye exams.
Some tele‑screening programs use artificial intelligence (AI) algorithms to detect signs of retinopathy automatically. For example, the FDA has approved AI tools that analyze retinal images for more than mild diabetic retinopathy. If the algorithm flags a suspicious image, patients are referred for a comprehensive eye exam. AI screening is not a substitute for an exam, but it can help identify at‑risk individuals who might otherwise go unscreened.
Screening recommendations
The American Diabetes Association (ADA) and other professional organizations provide clear guidelines for when people with diabetes should have eye exams:
- Type 1 diabetes: Have an initial comprehensive eye exam within five years of diagnosis. After that, schedule annual exams.
- Type 2 diabetes: Have a dilated eye exam at the time of diagnosis and then once every year.
- Pregnancy: Women with diabetes who are pregnant or planning to become pregnant should have an exam before conception, early in the first trimester and once every trimester thereafter. Gestational diabetes without retinopathy may not need frequent retinal screening but should follow general pregnancy diabetes care.
- No diabetic retinopathy: If no retinopathy is present and blood sugar is well‑controlled, your eye doctor might suggest exams every 1–2 years.
- Existing diabetic retinopathy: People with any level of retinopathy typically need annual or more frequent exams to monitor disease progression.
These guidelines highlight the importance of early detection; by the time symptoms appear, retinopathy may already be advanced.
Treatment options

Treating diabetic retinopathy aims to stop or slow disease progression and prevent vision loss. The right treatment depends on the stage of the disease and whether macular edema is present. Common options include:
Controlling blood sugar, blood pressure and cholesterol
The foundation of diabetic retinopathy management is good overall diabetes control. Keeping your A1C, blood pressure and cholesterol within target ranges can slow or even halt retinopathy progression. The NEI advises patients to maintain healthy eating habits, stay active and follow their doctor’s instructions for medication. Regular exercise and weight management improve blood sugar control and reduce cardiovascular risks.
Anti‑VEGF injections
In advanced NPDR, proliferative retinopathy or diabetic macular edema, intravitreal injections of anti‑vascular endothelial growth factor (anti‑VEGF) drugs are often the first‑line treatment. These medications (such as ranibizumab, aflibercept and bevacizumab) block the VEGF protein that promotes abnormal blood vessel growth and leakage. The AAO explains that anti‑VEGF injections can reduce swelling, prevent new vessel growth and improve vision. Patients usually need a series of injections spaced weeks apart. Over time the interval between injections may be extended.
Corticosteroid injections or implants
Steroid medications reduce inflammation and vascular leakage. They are sometimes used when anti‑VEGF therapy alone is insufficient or when DME does not respond. Corticosteroids may be injected directly into the eye or delivered via a slow‑release implant. Steroids can have side effects such as cataract formation and increased eye pressure, so doctors carefully monitor patients.
Laser therapy
Laser treatment has been a mainstay of diabetic retinopathy care for decades. There are two primary types:
- Focal/grid laser (photocoagulation) is used to treat localized areas of leakage in diabetic macular edema. Small laser burns seal leaking microaneurysms.
- Panretinal photocoagulation (PRP) treats proliferative retinopathy. Multiple laser burns are applied to the peripheral retina, reducing the retina’s oxygen demand and prompting abnormal vessels to shrink and disappear. PRP can preserve central vision but may cause side‑effects such as reduced peripheral or night vision.
Vitrectomy
A vitrectomy is a surgical procedure used for advanced cases when there is vitreous hemorrhage (bleeding into the gel inside the eye) or tractional retinal detachment. During vitrectomy, the surgeon removes the blood‑filled vitreous and may remove scar tissue pulling on the retina. The cavity is then filled with a clear solution. While more invasive, vitrectomy can restore vision if performed before permanent retinal damage occurs.
Combined treatments and follow‑up
Often, a combination of anti‑VEGF injections, laser therapy and surgery provides the best outcome. Treatment does not cure diabetic retinopathy, but it can prevent progression. The Cleveland Clinic stresses that early diagnosis and treatment can delay vision loss; there is no cure, but proper management is highly effective.
Living with diabetic retinopathy
Receiving a diagnosis of diabetic retinopathy can be frightening, but many people continue to live full lives with good vision. Managing diabetes and protecting your eyes requires commitment and teamwork with your healthcare providers. Here are practical steps:
- Monitor blood sugar regularly: Aim to keep your blood glucose within the target range set by your doctor. Check your A1C level at least twice a year (or as recommended). Keeping your A1C below 7 percent reduces the risk of diabetic complications.
- Control blood pressure and cholesterol: High blood pressure damages blood vessels throughout your body, including the retina. Follow your doctor’s guidelines for diet, exercise and medication.
- Maintain a healthy lifestyle: Eat a balanced diet rich in fruits, vegetables, whole grains and lean proteins. Limit refined sugars and saturated fats. Aim for at least 30 minutes of physical activity most days of the week.
- Quit smoking: Smoking accelerates vascular damage and increases the risk of complications. Seek support to quit if needed.
- Attend regular eye exams: Even if your vision seems fine, schedule dilated eye exams as recommended. Early detection allows timely treatment.
- Know the warning signs: Learn the symptoms of retinopathy and contact your eye doctor promptly if you notice floaters, blurred or distorted vision, dark spots or sudden vision changes.
- Coordinate care: Work closely with your primary care doctor, endocrinologist and eye specialist. Share test results and adjust treatment plans as needed.
By following these steps, many people can slow or prevent retinopathy progression. Keeping open communication with your healthcare team is key.
Research and emerging technologies
Rapid advances in science and technology are reshaping diabetic retinopathy care. Some notable developments include:
Tele‑ophthalmology programs
Tele‑ophthalmology uses retinal cameras placed in primary care clinics, pharmacies or community centers. A trained technician captures retinal images; then an eye specialist reviews the images remotely. In a large tele‑ophthalmology program at the Bascom Palmer Eye Institute, more than 7,000 telehealth encounters were completed for patients with acute eye concerns. The program reported that 96.5 % of telemedicine encounters were successfully completed using video conferencing. Such high success rates suggest telehealth can expand access, especially in rural areas or among people who have difficulty traveling to an ophthalmologist.
Artificial intelligence in screening and diagnosis
AI algorithms can analyze retinal images with accuracy comparable to eye specialists. The FDA‑approved systems mentioned earlier detect referable diabetic retinopathy and prompt referral for in‑person care. This technology is especially useful in resource‑limited settings where eye specialists are scarce. Professional organizations caution that AI should assist rather than replace clinicians; final decisions and patient counselling remain the responsibility of eye care professionals.
Pharmacologic advances
Beyond anti‑VEGF drugs, researchers are investigating agents that target additional pathways involved in retinopathy, such as inhibitors of protein kinase C, angiopoietin‑2 and integrins. Combination therapies may offer better control of leakage and neovascularization.
Gene therapy and regenerative medicine
Scientists are exploring gene therapy to deliver protective or anti‑angiogenic proteins directly to the retina. Other approaches use stem cells to replace damaged retinal cells. Though still experimental, these treatments could one day offer lasting solutions for advanced retinopathy.
Wearable glucose monitors and digital health tools
Continuous glucose monitors (CGMs) help people maintain tighter blood sugar control. Smartphone apps and digital coaching platforms support lifestyle changes and medication adherence. Better glucose control translates to lower risk of complications like retinopathy.
The pace of innovation suggests that care for diabetic retinopathy will continue to improve. However, technology can’t replace the basics: regular eye exams and careful management of diabetes and cardiovascular risk factors.
The global burden of diabetic retinopathy
Diabetic retinopathy is not just a medical issue; it’s a public health concern affecting millions. Some sobering statistics:
- Global prevalence: About 93 million people worldwide have diabetic retinopathy.
- Rising numbers: In 2020, an estimated 103 million people were living with the condition, and projections suggest 160 million cases by 2045.
- Vision‑threatening retinopathy: Of those with retinopathy, roughly 25–30 % develop diabetic macular edema.
- Economic impact: Visual impairment reduces work productivity and independence. Healthcare systems spend billions annually on treatment and support services.
- Inequities: People in low‑income countries often lack access to screening and treatment. Tele‑ophthalmology and AI could help bridge this gap.
These numbers highlight the urgent need for preventive care, early detection and accessible treatment. Diabetic retinopathy is the only major cause of blindness that has not decreased in prevalence since 1990. Coordinated public health efforts are essential to reduce this burden.
Preventing diabetic retinopathy – practical tips
While you can’t guarantee you’ll never develop diabetic retinopathy, you can significantly lower your risk. Consider these tips:
- Know your numbers: Monitor your blood sugar (fasting and post‑meal levels), A1C, blood pressure and cholesterol. Work with your doctor to set realistic targets.
- Healthy eating: Choose complex carbohydrates, lean proteins and healthy fats. Limit sugary drinks and processed snacks. Spread carbohydrates evenly across meals to avoid spikes.
- Stay active: Aim for at least 150 minutes of moderate exercise each week. Walking, swimming, cycling or dancing are great options. Exercise improves insulin sensitivity and cardiovascular health.
- Take medications as prescribed: Don’t skip doses of insulin or oral medications. If you’re having trouble affording or remembering medications, discuss alternatives with your healthcare team.
- Avoid smoking and limit alcohol: Smoking damages blood vessels and increases your risk of complications. If you drink alcohol, do so in moderation and account for its effect on blood sugar.
- Regular checkups: See your primary care doctor, endocrinologist and eye specialist regularly. Early detection and intervention make a big difference.
- During pregnancy: Work with your obstetrician and ophthalmologist if you have diabetes. Get eye exams early and regularly during pregnancy.
- Educate yourself: Learn about diabetic complications. Share information with family and friends who have diabetes. Awareness empowers you to take proactive steps.
Conclusion – take charge of your eye health
Diabetic retinopathy is a common and serious complication of diabetes, but it is not inevitable. By understanding what it is, who is at risk, how it progresses and how it’s treated, you can take proactive steps to protect your sight. Regular eye exams, good control of blood sugar, blood pressure and cholesterol, and healthy lifestyle choices are powerful tools to prevent or slow retinopathy.
As you’ve learned, technology like tele‑ophthalmology and AI is expanding access to screening and helping detect retinopathy earlier. Research into new drugs, gene therapies and regenerative medicine offers hope for even better treatments in the future. Still, the most important action remains simple: schedule your annual dilated eye exam and talk to your healthcare team about managing your diabetes. Early detection saves vision.
Understanding diabetic retinopathy is the first step. The next step is yours. Take charge of your eye health today, and encourage friends and family with diabetes to do the same.
{kind=link}